Inherited retinal diseases (IRDs) are, as their name suggests, inherited through families. The conditions are passed down through “Mendelian inheritance” – one of three different pathways (autosomal dominant, autosomal recessive or X-linked) – or through mitochondrial inheritance.
Four inheritance patterns associated with IRDs
1. Autosomal Recessive Inheritance Pattern
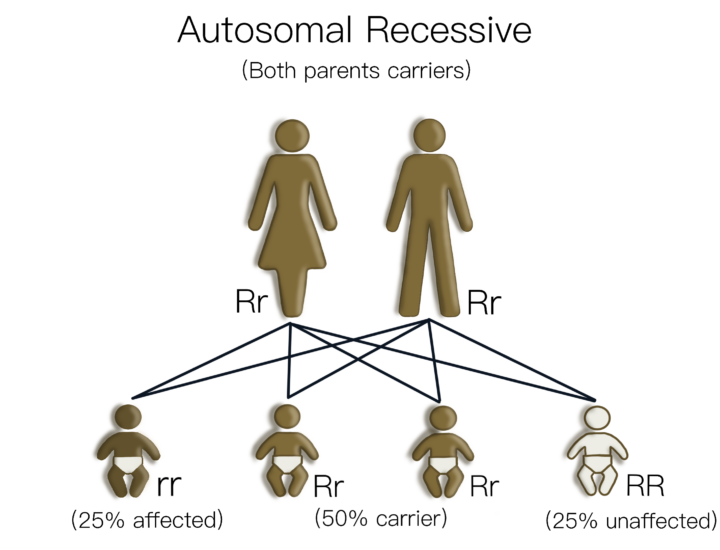
Autosomal recessive inheritance means each parent is a carrier but is not affected by the disease themselves. Each of their children will have a 25% chance of being affected, with males and females having an equal chance of being affected. The children have a 50% chance of being a carrier (having one healthy and one mutated copy of the gene).
The diagram on the right displays autosomal recessive inheritance where both parents are carriers. It shows how the recessive genes are passed from the two carrier parents to their children. The gene mutation is represented by “r” and the normal gene by “R”. A person will only have the disease if they have two copies of the gene mutation (rr). Carrier Mother Rr, Carrier Father Rr, Affected Child rr (25%), Carrier Child Rr (50%) x 2, Normal Child RR (25%).
This is the most common way in which the IRDs, retinitis pigmentosa and Leber congenital amaurosis, are inherited.
2. Autosomal Dominant Inheritance Pattern
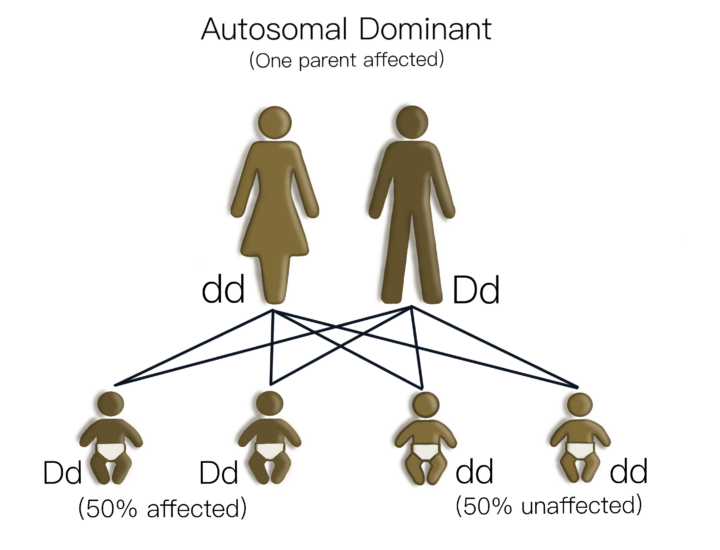
In autosomal dominant inherited retinal disease one parent is affected and each pregnancy has a 50% chance that the child will be affected. Males and females are equally affected. A person only needs one copy of the mutated gene to develop the IRD.
The diagram on the right indicates the four possible combinations of genetic information that may be passed on by the parents, when one is affected and the other not. The dominant gene anomaly is represented by “D” and the normal gene by “d”. It displays autosomal dominant inheritance where only one parent is affected – Normal Mother dd, Affected Father Dd, Affected Daughter Dd (25%), Affected Son Dd (25%), Normal Daughter dd (25%), Normal Son dd (25%)
3. X-linked Recessive Inheritance Pattern
In humans, a male has one X and one Y chromosome, and females have two X chromosomes. This means that a father will always pass his Y chromosome onto a son, and his X chromosome onto a daughter.
X-linked conditions are caused by gene mutations on the X-chromosome. X-linked inherited retinal diseases include choroideremia, juvenile retinoschisis and X-linked retinitis pigmentosa.
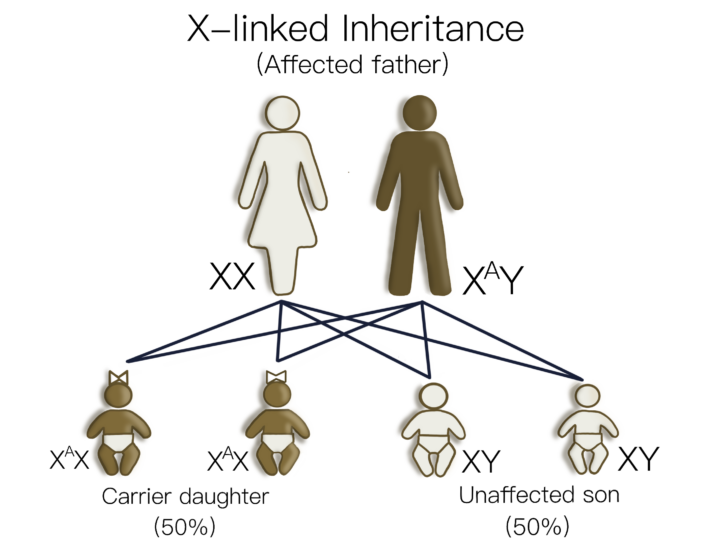
In these conditions, an affected male and an unaffected female will have unaffected sons and carrier daughters.
The diagram on the top right displays this X-linked Recessive Inheritance with a Normal Mother XX, Affected Father XaY, with all daughters as carriers XaX and all sons unaffected XY.
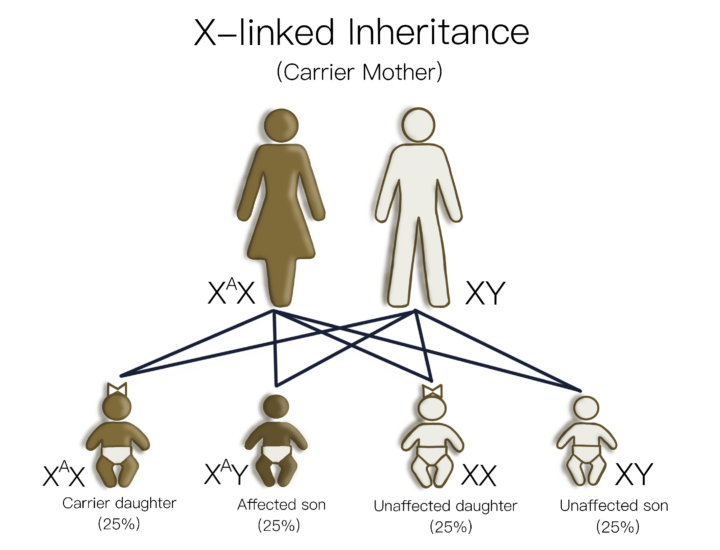
In another example, a carrier female with an unaffected male will produce children with a 50% chance that each son will have the inherited retinal disease. There is also a 50% probability that each daughter will be a carrier.
The diagram on the bottom right displays this type of X-linked Recessive Inheritance with a Carrier Mother XaX, Father XY, Carrier Daughter XaX (25%), Affected Son XaY (25%) Normal Daughter XX (25%), Normal Son XY (25%).
Female carriers of an X-linked IRD can have variable symptoms. Many women will not experience vision loss, nor show significant clinical signs of the IRD. However, others can develop retinal changes and vision loss, even to the stage of legal blindness. It is important that female carriers of X-linked IRDs also have regular eye examinations in order to monitor their eye health and vision over time.
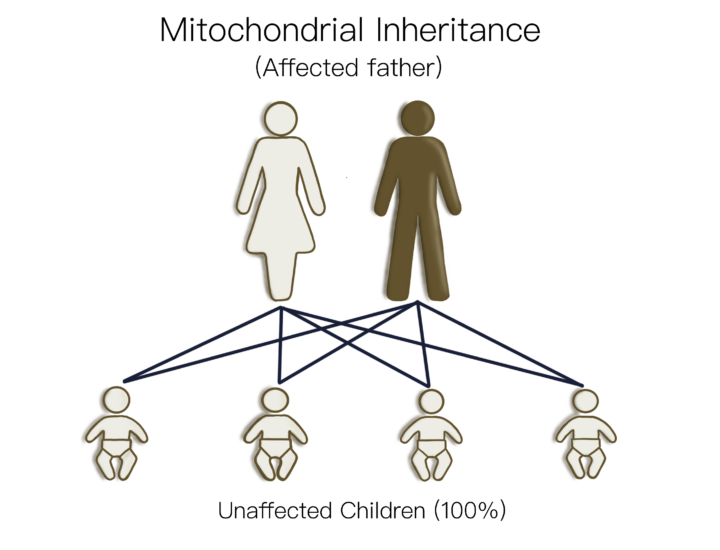
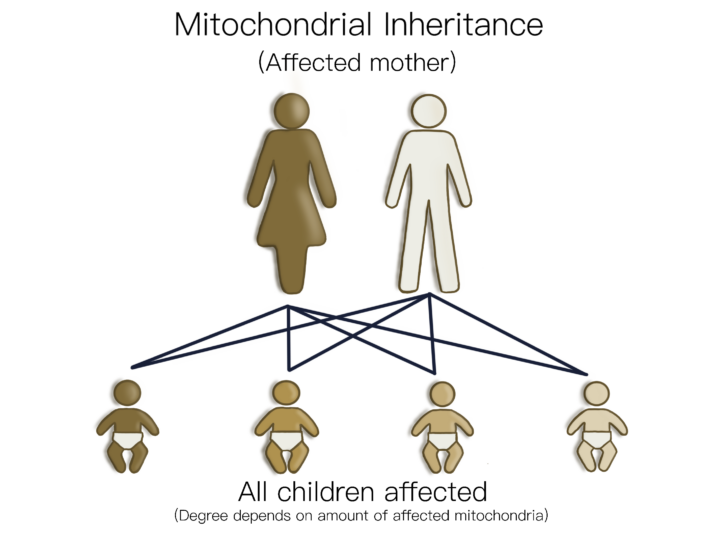
4. Mitochondrial Inheritance
The Mendelian inheritance patterns highlighted above describe how genes that are found in the nuclear DNA of a cell are passed on. These are the most common ways in which an IRD will be inherited. However, in some cases, the gene mutation is found in another compartment of the cell, called the mitochondria.
Mitochondria are the “energy powerhouse” of the cell, where energy from our food is converted into energy which the cells can use to function.
Mitochondrial DNA is composed of special genes that help in this energy production so, when there is a mutation, the cell does not have enough energy to function properly.
In the eye, this can lead to a number of inherited retinal diseases including Leber Hereditary Optic Neuropathy (LHON). 1
All of a person’s mitochondria is inherited from their mother. This means that an affected male will not pass the condition on to their children.
The impact of a mitochondrial gene function can be very variable, as every cell has different numbers of mitochondrial units. For example, in a cohort of people with a known LHON gene mutation, only 17.5% of males and 5.4% of females experienced vision loss. 2
First time mutation
Sometimes people can have a “de novo” mutation, which means that the change in the gene has only occurred in them and has not been inherited.
Genetic testing
There are currently over 300 known genes that can cause IRDs. These genes are complex – sometimes the same gene can cause different clinical presentations and, vice versa, different genes can lead to the same clinical features.
Genetic testing and a family history can help identify the genetic cause of an IRD in around 60% of people 3 , but there are still many for whom the answer cannot currently be found. This is because we still do not know all the genes that cause IRDs and, in some cases, our testing is not sensitive enough to detect certain changes in the genetic information.
The complexity of inheritance of IRDs means that management of an IRD often will require a clinical geneticist and a genetic counsellor.